



A child’s facial growth, jaw development, and tooth alignment can offer early clues to breathing problems long before symptoms are easy to recognize.
Identifying these patterns at the right time allows orthodontic care to be thoughtfully planned—supporting healthier breathing, guiding proper facial growth, and contributing to a team-based approach focused on lasting airway and overall health.
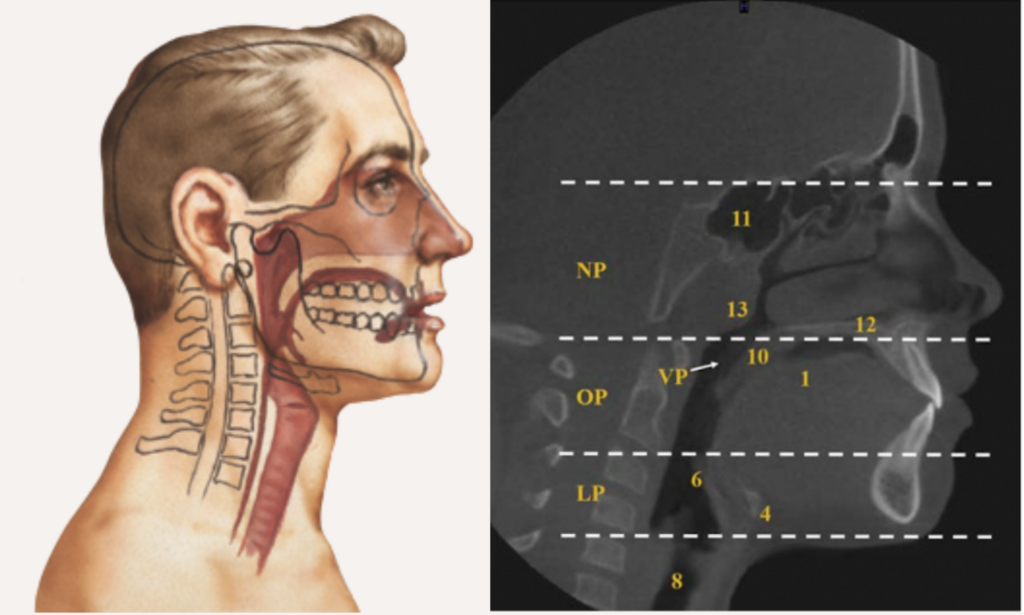
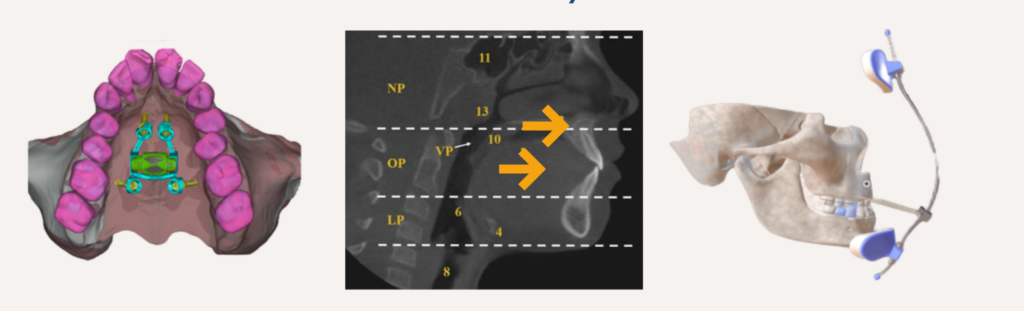
AIRWAY ANATOMY: 3 SEGMENTS
Nasopharynx (NP)
between nares and hard palate
Oropharynx (OP)
soft palate to upper border of epiglottis
Laryngopharynx (LP)
base of tongue to inferior border of cricoid cartilage
Early identification of children at risk of SDB is essential to prevent long-term health issues:
- cardiovascular/metabolic problems,
- growth impairment,
- cognitive/mood disturbances, and
- reduced quality of life.
Sleep-disordered breathing has multifactorial risk factors.
It may be related to:
-
Enlargement of soft tissue structures (such as the tonsils, adenoids, or tongue),
-
Constriction or underdevelopment of hard tissue structures (such as a narrow maxilla or retrusive jaws), and
-
Impaired neuromuscular control of the upper airway.
How does Orthodontics play a role in this?
Developmental modifications(role of orthodontics) in craniofacial structures can markedly influence airway size and stability.
craniofacial phenotypes that contribute to paediatric OSA
Class II with retrognathic mandible (Short Lower Jaw)
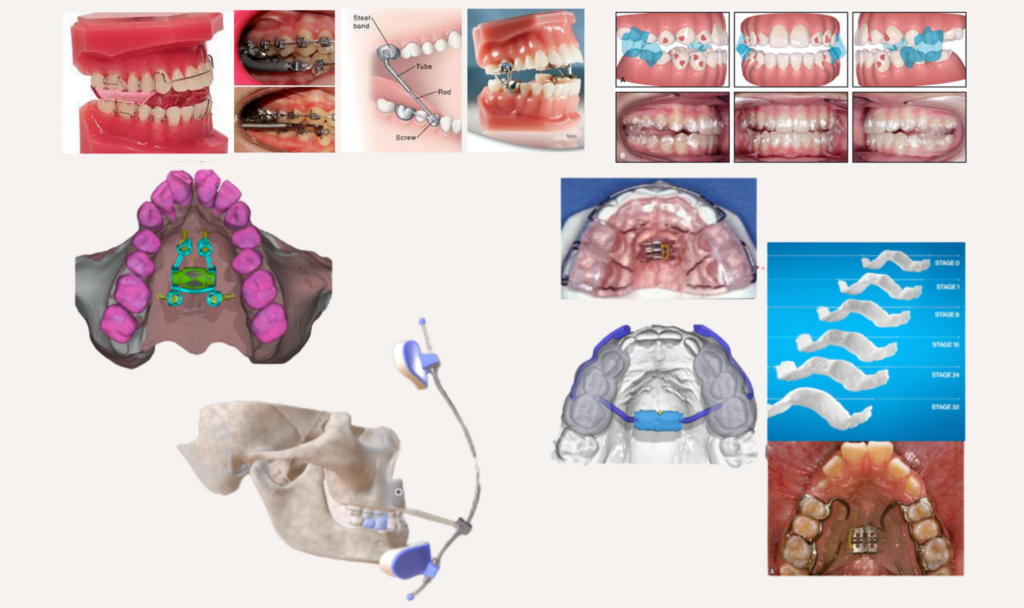
What can be done:
- Use functional appliances (FA) to advance the mandible forward.
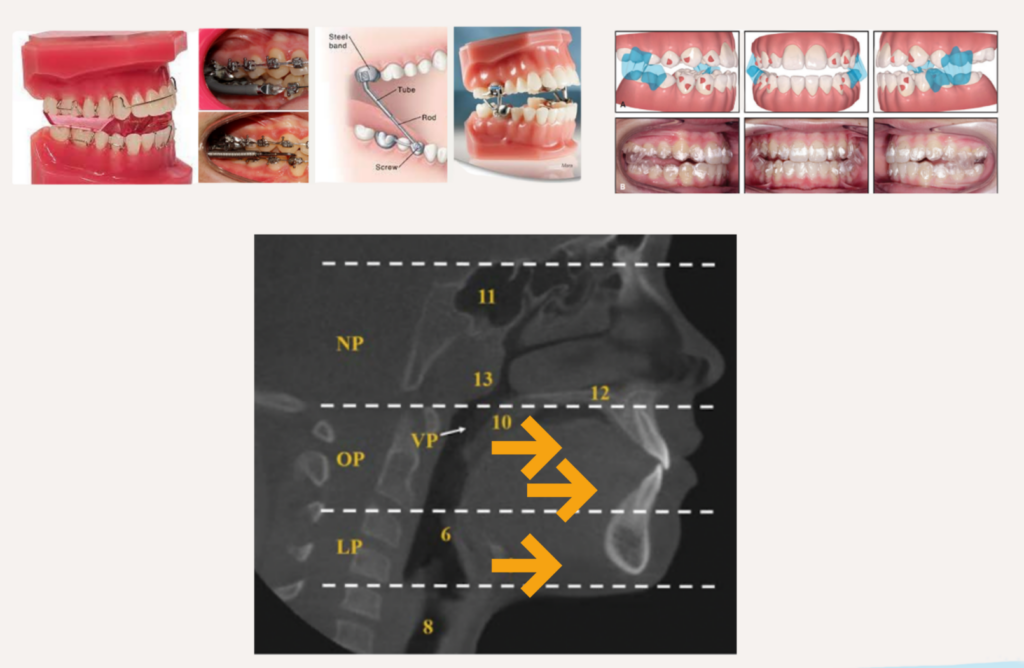
How can they improve the airway?
- Stretches tongue and suprahyoid muscles→ enlarges pharyngeal airway.
- Moves tongue away from soft palate→ anterior repositioning of soft palate.
Best timing?
- Most effective 1–2 years before pubertal growth peak, including pubertal growth spurt.
Evidence
- Airway improvements: small to moderate in upper pharynx.
- Functional improvement: short-term reduction in AHI, increase in SaO2.
- Evidence is promising but variable due to study differences; long-term stability not fully validated.
- Relies on individual biological responsiveness of condylar cartilage for supplementary mandibular growth’
Class III with retrognathic maxilla (Small/Flat Midface)
What can be done:
- Facemask therapy + RPE:(advances the maxilla forward and downward)
- Bone-anchored intermaxillary traction / MARPE
How can they improve the airway?
- Increases nasopharyngeal and post-palatal airway dimensions.
- Moves soft palate forward → improves upper airway space.
- Conventional facemask limited by mandibular rotation; bone-anchored methods counteracts adverse effects of mandibular rotation for better airway outcomes.
Evidence
- Early maxillary protraction shows more favorable skeletal and airway outcomes.
- Evidence supports short-term reduction in OSA severity and long-term craniofacial improvements.
Best timing?
- Ages 6–9: facemask + RPE for Class III with retrognathic maxilla.
- Ages 10–11: MARPE + facemask more effective
- Ages 12–15: bone-anchored mini-implants or mini-plates for severe discrepancies or advanced skeletal maturation.
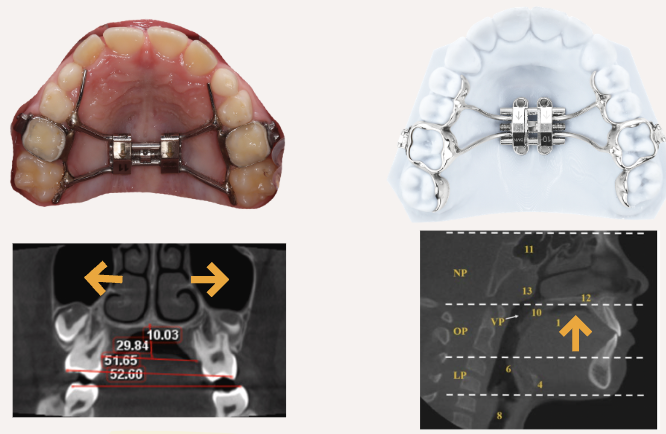
Nasomaxillary complex contriction (Narrow Upper Jaw)
What can be done:
- Rapid Palatal Expansion (RPE): widens maxillary arch→ reshapes nasal cavity.
- TAD-supported expansion (MARPE): more stable, skeletal-based expansion.
How can they improve the airway?
- Increases nasal volume, reduces nasal resistance→ improves nasal airflow.
- Decreases negative pressure during breathing→ better ventilation
- Supports forward/upward tongue positioning→ improves oropharyngeal dimensions.
Evidence
- RPE reported to reduce AHI in children with OSA, with effects maintained over 3 months -14 years follow-up.
- MARPE demonstrates superior improvements over conventional RPE in nasal airflow, reduced airway resistance, and increased upper airway dimensions.
Best timing?
- Ages 5–6 years if severe nasal obstruction
- Ages 6–9: standard RPE effective
- Ages 10–11: consider TAD-assisted expansion for severe cases.
Conclusion
Early orthodontic intervention aims to increase hard tissue volume to support better nasal and upper airway space during growth.
However, airway disorders are multifactorial in nature. Early orthodontic treatment should not be viewed as a primary or standalone solution for breathing issues.
A comprehensive, multidisciplinary evaluation is essential to accurately determine the site and cause of obstruction before any treatment is planned.
At MyBracesClinic, we do not initiate early orthodontic treatment purely for airway concerns in the absence of clear skeletal or dental indications. Instead, we collaborate closely with Dr Shaun Loh, , an ENT specialist at Gleneagles Hospital, to:
Diagnose conditions such as obstructive sleep apnea (OSA)
Assess nasal and upper airway resistance
Determine whether early intervention may be appropriate as an adjunctive treatment within a broader airway management plan
Our approach ensures that any orthodontic intervention is part of a carefully coordinated, evidence-based strategy — not an isolated attempt to manage a complex medical condition.
If you think early intervention might be right for you or your child, book a consultation with us—we’ll be happy to guide you through the options.